


New ambulances don’t pay for themselves
Some math on emergency response and ambulance fees

As a reminder, we’re hosting a meetup today. Hope you can join us at 5:30 at the Berghoff. More details here.
One of the main takeaways from my last post on the Chicago Fire Department was our need for more ambulances. Our current fleet of 80 is simply not sufficient to meet Chicago’s EMS needs, and meeting the Firefighters’ Union’s proposal for another 20 would be a big help.
But it’s important to pay for the things we need, too, and ambulances are no exception. Because the city bills individuals for ambulance rides to the ER - which generates revenue - I’ve come across a few instances of people arguing that new ambulances could pay for themselves. A Tribune story this week cites CFU President Pat Cleary as “contend[ing] additional ambulances would make the city money.” That’s consistent with what he told WBBM last October as well.
To be blunt, I don’t think the math checks out.
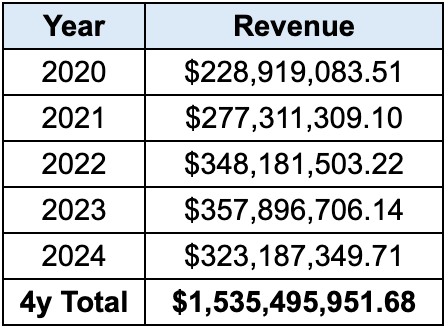
First, here’s what is definitely true: these fees are a real revenue generator for the city. Over the past five years, we’ve collected an average of roughly $300 million in ambulance fee revenue every year. For comparison, the entire 2024 EMS personnel budget was about $82 million1 - so that’s a big net benefit to the city!
What’s much less clear, however, is whether this is scalable to *new* ambulances. The basic question here is whether the extra revenue an additional ambulance brings in would exceed the cost of running that ambulance. That math isn’t hard to run through if we make some ballpark assumptions.
The math part
Start with the cost side. As we covered previously, a new ambulance probably costs somewhere around $250,000. Amortize that over ten years and we need to cover $25,000 in ambulance cost per year (before borrowing costs). A far bigger expense, however, is staffing. Each ambulance has a two-man crew - a paramedic and paramedic-in-charge - and based on the last CBA, the lowest possible cost for that crew is around $140,0002 for the pair. Chicago paramedics work on a 24/72 schedule (one 24-hour shift on followed by three 24-hour shifts off), meaning you’d need four crews to keep that ambulance fully staffed. That brings our total cost to $585,000 for the year ($140k x 4 crews, plus 25k for the amortized vehicle cost). I’m ignoring smaller costs like maintenance and gas (and bigger costs like employees’ pension expenses), but it’s a start.
Now the revenue side. Per the city’s website, Chicago charges $2,820 for an advanced life support (ALS) ambulance ride, plus $19 per mile and an additional $28 if they provide oxygen to the passenger. Over the past five years, that’s worked out to an average gross charge of $2,925.54 per ride.
But the amount we actually collect is a lot lower than that. Here’s a more detailed look at annual collection data from the city’s Department of Revenue:

Right off the bat, ‘contractual adjustments’ - a fancy way of saying “how much Medicare, Medicaid, or private health insurers are actually willing to pay for an ambulance ride” - reduce that gross charge by over 35%, leaving us with an average net charge of about $1880. On top of that, the city doesn’t do a great job collecting on its debts. Over the past five years, we’ve only actually collected about 64% of the net ambulance fee charges we’ve made. That takes us to an average of around $1200 in actual fee revenue collected per ambulance ride.
Assuming $1200 in revenue per ride and $585,000 in costs per year, each ambulance needs to make about 490 new trips per year to break even. Is that feasible?
We need to know how many EMS medical incidents aren’t being met by an ambulance. To do that, I requested data from the Office of Emergency Management and Communications (OEMC) on all 911 medical emergencies from the last few years. They were eventually nice enough to respond3 with some meaty data files including information on around 1.4 million medical responses over 2021 to 2024. In 11,101 of those cases, no ambulances were listed as responding units. That’s about 2,800 cases per year, and it’s probably a good ballpark estimate on the ‘unmet caseload’ we could expect our larger fleet to help us with.
That’s not nothing, but it would only offset the cost of 5 or 6 new ambulances, not 20. Unless you assume that having more ambulances will convince a lot more people to start calling 911 for a hospital ride, there’s simply not enough “new demand” here to generate revenue.
… and that’s okay
To be clear - that’s fine! The purpose of CFD ambulances is not to make money for the city - that would be an insane way to run EMS response. The purpose is to provide emergency medical care and save lives.
By that same token, whether we get more ambulances should not be about whether doing so would generate more revenue to the city. Instead, what those 20 ambulances would absolutely, positively, 100% definitely do is let us respond more quickly to the incidents our paramedics are facing today. Those faster response times are intrinsically good in and of themselves. The fact that the fee revenue won’t pay for them doesn’t change that.
It does, however, mean that we’ll need to find some other way to pay for the larger fleet - which might be why Cleary wants to contend differently. In some ways, this is a new twist on a familiar theme for Chicago fiscal issues4 - we look for easy solutions instead of acknowledging the real tradeoffs and tough choices we have to make.
As I argued before, the easiest way to pay for a larger ambulance service is shifting firefighter/paramedics over to ambulance staffing, which would generate significant paramedic overtime savings. But doing that would mean cuts to the fire suppression side which the union would obviously fight tooth and nail. That’s their prerogative, of course, but it doesn’t mean they’re right - and it doesn’t change the actual math, either.
See Appendix B (beginning on page 103) of the CFU collective bargaining agreement here. I’m using the 2021 salary table (page 108), since that’s the latest. Paramedics follow the F1 schedule; PICs follow the F3A Schedule. The Step 1 salaries for both are $62,160 and $78,366, respectively, or $140,526 overall. It’s obviously worth pointing out those are lowball estimates - most of the employees we’d staff the ambulances with are not brand new (and I was arguing for FF/PM restaffing - those cross-trained employees carry a higher salary scale than paramedics do, too). In the city’s 2024 budget, the average budgeted salary for an EMS employee was around $102,712, which would take our total labor cost north of $820k per year, for what it’s worth.
In case it is useful to anyone for any reason: this was FOIA Request #F251187-013025 to the OEMC through the city’s online portal.
I’m reminded of the frustrating debate we covered in December around “vacancy cuts” as an (alleged) form of budget cost savings.
One way to pay is to eliminate overstaffing. Your previous posted noted that the CFD's contract mandates a five man crew on engines. The industry standard is a four man crew (and any number of departments only have three). I would think a "fair contract" would do things like eliminating any form of overstaffing requirements.
Where does the estimate that we need another 20 ambulances come from? I’m trying to reconcile that claim with the idea that there’s not enough unmet demand to pay for them. Is demand uneven enough that we are sometimes 20 short even though each new ambulance would get less than two calls a day? Or is this planning for reserve capacity for worst case mass casualty scenarios?